


Most of us know that we can reduce our risk of disease by eating a healthy diet, getting enough exercise, and not smoking. But, did you know that your family history might be one of the strongest influences on your risk of developing heart disease, stroke, diabetes, or cancer? Even though you cannot change your genetic makeup, knowing your family history can help you reduce your risk of developing health problems.
Family members share their genes, as well as their environment, lifestyles, and habits. Everyone can recognize traits such as curly hair, dimples, leanness, or athletic ability that run in their families. Risks for diseases such as asthma, diabetes, cancer, and heart disease also run in families. Everyone’s family history of disease is different. The key features of a family history that may increase risk are:
- Diseases that occur at an earlier age than expected (10 to 20 years before most people get the disease)
- Disease in more than one close relative
- Disease that does not usually affect a certain gender (for example, breast cancer in a male)
- Certain combinations of diseases within a family (for example, breast and ovarian cancer, or heart disease and diabetes)
If your family has one or more of these features, your family history may hold important clues about your risk for disease. People with a family history of disease may have the most to gain from lifestyle changes and screening tests. You cannot change your genes, but you can change unhealthy behaviors such as smoking, inactivity, and poor eating habits. In many cases, adopting a healthier lifestyle can reduce your risk for diseases that run in your family. Screening tests (such as mammograms and colorectal cancer screening) can detect diseases like cancer at an early stage, when they are most treatable. Screening tests can also detect disease risk factors like high cholesterol and high blood pressure, which can be treated to reduce the chances of getting a disease.
Learning About Your Family History
To learn about your family history:
- Ask questions
- Talk at family gatherings
- Look at death certificates and family medical records, if possible
Collect information about your grandparents, parents, aunts, uncles, nieces, nephews, siblings, and children. The type of information to collect includes:
- Major medical conditions and causes of death
- Age of disease onset and age at death
- Ethnic background
Write down the information and share it with your doctor. Your doctor will:
- Assess your disease risk based on your family history and other risk factors
- Recommend lifestyle changes to help prevent disease
- Prescribe screening tests to detect disease early
If your doctor notices a pattern of disease in your family, it may be a sign of an inherited form of disease that is passed on from generation to generation. Your doctor may refer you to a specialist who can help determine if you have an inherited form of disease. Genetic testing may also help determine if you or your family members are at risk. Even with inherited forms of disease, steps can be taken to reduce your risk.
What If You Don’t Uncover a Family History of Disease?
Being aware of your family health history is an important part of a lifelong wellness plan. Even if you don’t have a history of a particular health problem in your family, you could still be at risk. This is because:
- Your lifestyle, personal medical history, and other factors influence your chances of getting a disease
- You may be unaware of disease in some family members
- You could have family members who died young, before they had a chance to develop chronic conditions such as heart disease, stroke, diabetes, or cancer
Resources & References
Understanding Genetics: A New York, Mid-Atlantic Guide for Patients and Health Professionals > View or Download the .PDF
- Understanding Genetics: A New York, Mid-Atlantic Guide for Patients and Health Professionals. https://www.ncbi.nlm.nih.gov/books/NBK115560/
- Centers for Disease Control and Prevention. Family history is important for health. www.cdc.gov/genomics/public/famhix/fs.htm.
- Centers for Disease Control and Prevention, National Office of Public Health Genomics www.cdc.gov/genomics.
- Genetic Alliance www.geneticalliance.org/familyhealthhistory.
- National Society of Genetic Counselors www.nsgc.org/consumer/familytree.
- U.S. Surgeon General’s Family History Initiative www.hhs.gov/familyhistory.
The incidence of chronic disease is increasing along with healthcare related costs. The functional medicine model of care provides a unique operating system to reverse illness, promote health, and optimize function.
This model of care demonstrates beneficial and sustainable associations with patient’s health-related quality of life (HRQoL).
A retrospective cohort study was performed to compare 7252 patients aged 18 years or older treated in a functional medicine setting with propensity score (PS)–matched patients in a primary care setting. Sensitivity analyses assessed improvement limited to patients seen at both 6 and 12 months. The study included patients who visited the Cleveland Clinic Center for Functional Medicine or a Cleveland Clinic family health center between April 1, 2015, and March 1, 2017.
Resources & References
Functional Medicine quality of life study > View or Download the .PDF

Should you use protein powders? It’s complicated.
“Is it better to get your nutrition from whole foods? Absolutely,” says Rebecca Mohning, a dietitian in the Washington area and owner of expertnutrition.net. Whole foods often include fiber, which helps regulate the digestive system, and vitamins, which help boost the immune system, and real foods generally are more balanced — they have a little bit of everything. (A cup of brown rice, for example, has fiber, protein, potassium and vitamins.)
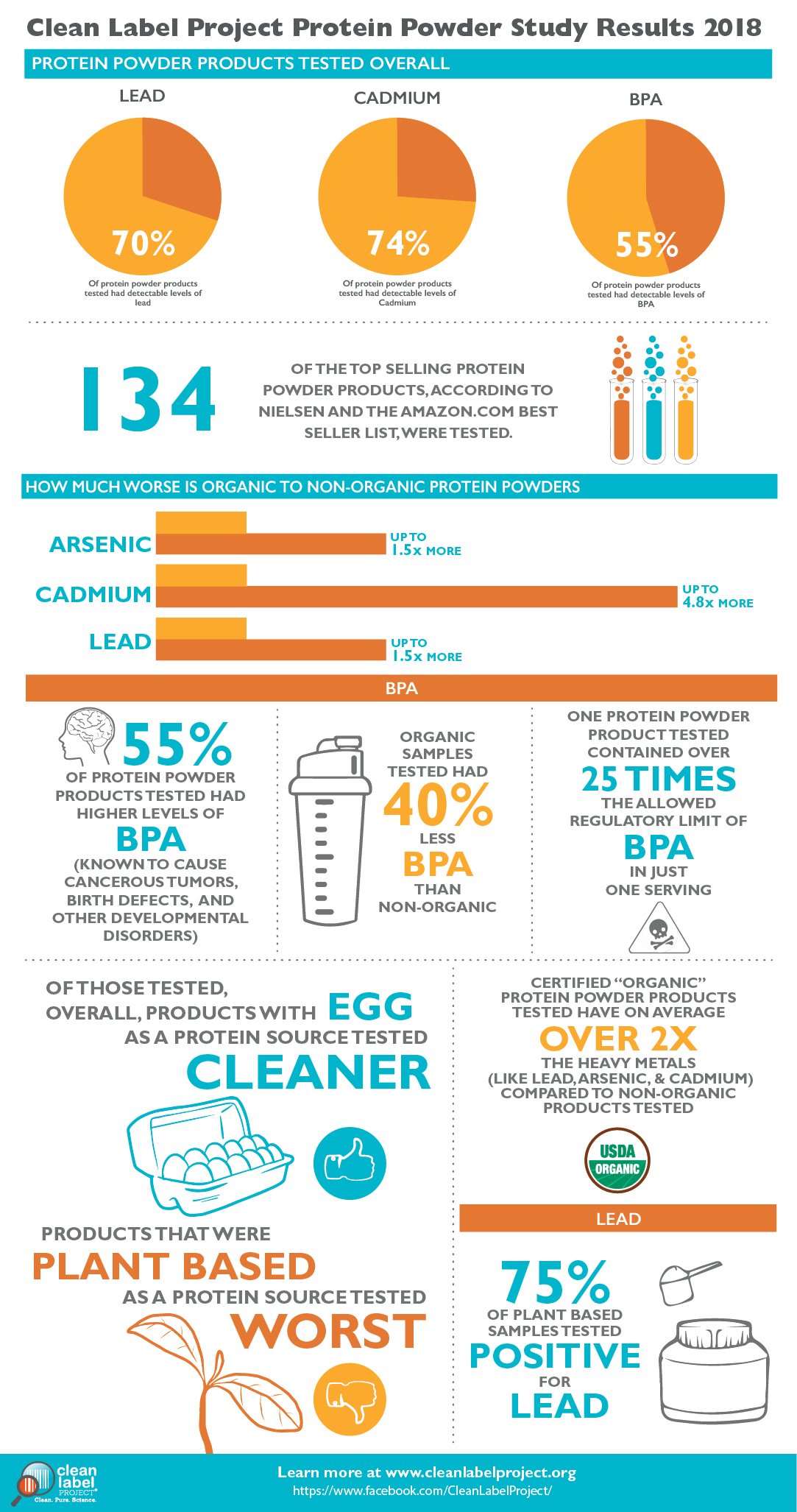
Protein Powder Study
The Clean Label Project™ completed a study of 134 protein powder products from 52 brands. Products were screened for over 130 toxins including heavy metals, BPA, pesticides, and other contaminants with links to cancer and other health conditions.
Resources & References
- Should you use protein powders? It’s complicated. > https://www.washingtonpost.com/lifestyle/wellness/should-you-use-protein-powders-its-complicated/2017/09/29/843d9d84-9e1c-11e7-8ea1-ed975285475e_story.html
- The Clean Label Project. > https://www.cleanlabelproject.org/protein-powder/
- Should You Have a Protein Shake Before or After Your Workout? > https://www.healthline.com/nutrition/protein-shake-before-or-after-workout#pre-vs-post-workout
- The hidden dangers of protein powders. > https://www.health.harvard.edu/staying-healthy/the-hidden-dangers-of-protein-powders


Put off the dentist and your smile isn’t the only thing that can suffer: Poor oral hygiene could hurt your heart health, suggests a new study from Finland.
After examining the teeth and the arteries of more than 500 people, the researchers discovered that those need of a root canal were nearly 3 times more likely to have acute coronary syndrome—a clogging of the heart’s arteries that can cause a heart attack—than patients with healthy teeth.
Bacteria from the tooth infection may spread to other parts of the body including the heart. What was not studied and possibly of greater import was the level of inflammation in the body as measured by inflammatory proteins in the blood. At higher levels, c-reactive proteins indicate a high level of inflammation which in turn is associated with many systemic diseases, not just heart disease. An unclean or infected mouth will raise the level of c-reactive proteins in the blood. It’s imperative to maintain your oral hygiene and keep up with your cleanings.

Resources & References
- Association of Endodontic Lesions with Coronary Artery Disease > https://journals.sagepub.com/doi/abs/10.1177/0022034516660509

Saturated fat does not clog the arteries: coronary heart disease is a chronic inflammatory condition, the risk of which can be effectively reduced from healthy lifestyle interventions.
Aseem Malhotra1, Rita F Redberg2,3, Pascal Meier4,5
Coronary artery disease pathogenesis and treatment urgently requires a paradigm shift. Despite popular belief among doctors and the public, the conceptual model of dietary saturated fat clogging a pipe is just plain wrong. A landmark systematic review and meta-analysis of observational studies showed no association between saturated fat consumption and (1) all-cause mortality, (2) coronary heart disease (CHD), (3) CHD mortality, (4) ischaemic stroke or (5) type 2 diabetes in healthy adults.1 Similarly in the secondary prevention of CHD there is no benefit from reduced fat, including saturated fat, on myocardial infarction, cardiovascular or all-cause mortality.2 It is instructive to note that in an angiographic study of postmenopausal women with CHD, greater intake of saturated fat was associated with less progression of atherosclerosis whereas carbohydrate and polyunsaturated fat intake were associated with greater progression.3
Preventing the development of atherosclerosis is important but it is atherothrombosis that is the real killer
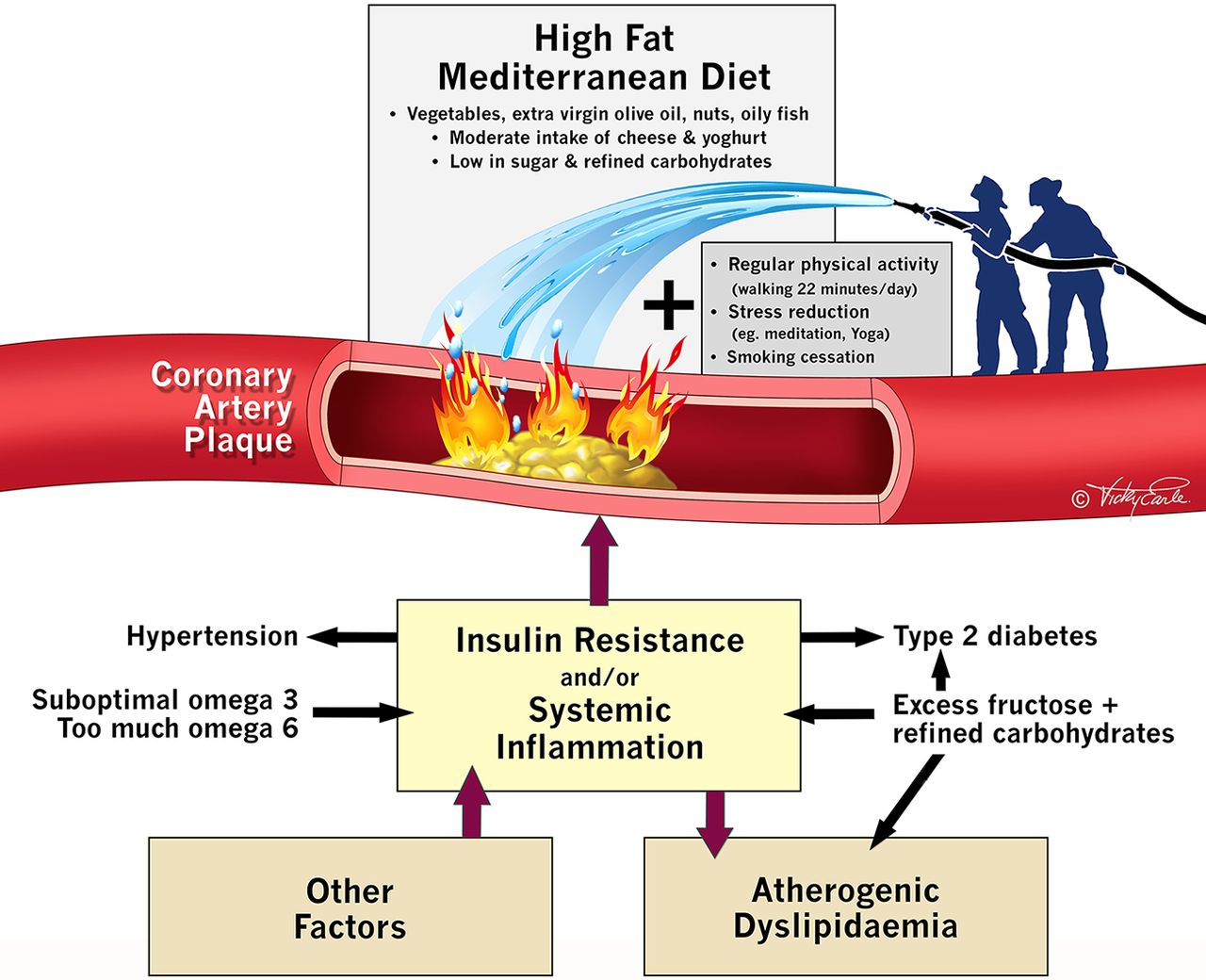
The inflammatory processes that contribute to cholesterol deposition within the artery wall and subsequent plaque formation (atherosclerosis), more closely resembles a ‘pimple’ (figure 1). Most cardiac events occur at sites with <70% coronary artery obstruction and these do not generate ischaemia on stress testing.4 When plaques rupture (analogous to a pimple bursting), coronary thrombosis and myocardial infarction can occur within minutes. The limitation of the current plumbing approach (‘unclogging a pipe’) to the management of coronary disease is revealed by a series of randomised controlled trials (RCTs) which prove that stenting significantly obstructive stable lesions fail to prevent myocardial infarction or to reduce mortality.5
Dietary RCTs with outcome benefit in primary and secondary prevention
In comparison with advice to follow a ‘low fat’ diet (37% fat), an energy-unrestricted Mediterranean diet (41% fat) supplemented with at least four tablespoons of extra virgin olive oil or a handful of nuts (PREDIMED) achieved a significant 30% (number needed to treat (NNT)=61) reduction in cardiovascular events in over 7500 high-risk patients. Furthermore, the Lyon Heart study showed that adopting a Mediterranean diet in secondary prevention improved hard outcomes for both recurrent myocardial infarction (NNT=18) and all-cause mortality (NNT=30), despite there being no significant difference in plasma low-density lipoprotein (LDL) cholesterol between the two groups. It is the alpha linoleic acid, polyphenols and omega-3 fatty acids present in nuts, extra virgin olive oil, vegetables and oily fish that rapidly attenuate inflammation and coronary thrombosis.6 Both control diets in these studies were relatively healthy, which make it highly likely that even larger benefits would be observed if the Mediterranean diets discussed above were compared with a typical western diet.
LDL cholesterol risk has been exaggerated
Decades of emphasis on the primacy of lowering plasma cholesterol, as if this was an end in itself and driving a market of ‘proven to lower cholesterol’ and ‘low-fat’ foods and medications, has been misguided. Selective reporting may partly explain this misconception. Reanalysis of unpublished data from the Sydney Diet Heart Study and the Minnesota coronary experiment reveal replacing saturated fat with linoleic acid containing vegetable oils increased mortality risk despite significant reductions in LDL and total cholesterol (TC).7
A high TC to high-density lipoprotein (HDL) ratio is the best predictor of cardiovascular risk (hence this calculation, not LDL, is used in recognised cardiovascular risk calculators such as that from Framingham). A high TC to HDL ratio is also a surrogate marker for insulin resistance (ie, chronically elevated serum insulin at the root of heart disease, type 2 diabetes and obesity). And in those over 60 years, a recent systematic review concluded that LDL cholesterol is not associated with cardiovascular disease and is inversely associated with all-cause mortality.8 A high TC to HDL ratio drops rapidly with dietary changes such as replacing refined carbohydrates with healthy high fat foods.
A simple way to combat insulin resistance (chronically high levels of serum insulin) and inflammation
Compared with physically inactive individuals, those who walk briskly at or above 150 min/week can increase life expectancy by 3.4–4.5 years independent of body weight.9 Regular brisk walking may also be more effective than running in preventing coronary disease. And just 30 min of moderate activity a day more than three times/week significantly improves insulin sensitivity and helps reverse insulin resistance (ie, lowers the chronically elevated levels of insulin that are associated with obesity) within months in sedentary middle-aged adults. This occurs independent of weight loss and suggests even a little activity goes a long way.
Another risk factor for CHD is environmental stress. Childhood trauma can lead to an average decrease in life expectancy of 20 years. Chronic stress increases glucocorticoid receptor resistance, which results in failure to down regulate the inflammatory response. Combining a complete lifestyle approach of a healthful diet, regular movement and stress reduction will improve quality of life, reduce cardiovascular and all-cause mortality.10 It is time to shift the public health message in the prevention and treatment of coronary artery disease away from measuring serum lipids and reducing dietary saturated fat. Coronary artery disease is a chronic inflammatory disease and it can be reduced effectively by walking 22 min a day and eating real food. There is no business model or market to help spread this simple yet powerful intervention.
Resources & References
Download a .PDF version of this article here.
- ↵de Souza RJ , Mente A , Maroleanu A , et al . Intake of saturated and trans unsaturated fatty acids and risk of all cause mortality, cardiovascular disease, and type 2 diabetes: systematic review and meta-analysis of observational studies. BMJ 2015;351:h3978.doi:10.1136/bmj.h3978 Abstract/FREE Full TextGoogle Scholar
- ↵Schwingshackl L , Hoffmann G . Dietary fatty acids in the secondary prevention of coronary heart disease: a systematic review, meta-analysis and meta-regression. BMJ Open 2014;4:e004487.doi:10.1136/bmjopen-2013-004487 Google Scholar
- ↵Mozaffarian D , Rimm EB , Herrington DM . Dietary fats, carbohydrate, and progression of coronary atherosclerosis in postmenopausal women. Am J Clin Nutr 2004;80:1175–84.Abstract/FREE Full TextGoogle Scholar
- ↵Rothberg MB . Coronary artery disease as clogged pipes: a misconceptual model. Circ Cardiovasc Qual Outcomes 2013;6:129–32.doi:10.1161/CIRCOUTCOMES.112.967778 FREE Full TextGoogle Scholar
- ↵Malhotra A . The whole truth about coronary stents: the elephant in the room. JAMA Intern Med 2014;174:1367–8.doi:10.1001/jamainternmed.2013.9190 Google Scholar
- ↵Chakrabarti S , Freedman JE . Review: nutriceuticals as antithrombotic agents. Cardiovasc Ther 2010;28:227–35.doi:10.1111/j.1755-5922.2010.00161.x CrossRefPubMedGoogle Scholar
- ↵Ramsden CE , Zamora D , Majchrzak-Hong S , et al . Re-evaluation of the traditional diet-heart hypothesis: analysis of recovered data from Minnesota coronary experiment (1968-73). BMJ 2016;353:i1246.doi:10.1136/bmj.i1246 Abstract/FREE Full TextGoogle Scholar
- ↵Ravnskov U , Diamond DM , Hama R , et al . Lack of an association or an inverse association between low-density-lipoprotein cholesterol and mortality in the elderly: a systematic review. BMJ Open 2016;6:e010401.doi:10.1136/bmjopen-2015-010401 Google Scholar
- ↵Moore SC , Patel AV , Matthews CE , et al . Leisure time physical activity of moderate to vigorous intensity and mortality: a large pooled cohort analysis. PLoS Med 2012;9:e1001335.doi:10.1371/journal.pmed.1001335 CrossRefPubMedGoogle Scholar
- ↵Blackburn EH , Epel ES . Too toxic to ignore. Nature 2012;490:169–71.CrossRefPubMedWeb of ScienceGoogle Scholar
Copyright Information:
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Britain’s leading anti-sugar campaigner and one of the most prolific doctors in the world influencing obesity thinking and highlighting the harms of too much medicine.
In addition to being a Consultant Cardiologist, Dr Malhotra is a member of the board of trustees of UK health think tank, The King’s Fund and a member of the Academy of Medical Royal Colleges Choosing Wisely Steering Group.
Here’s the link to his website: doctoraseem.com/biography/

